












WHAT A THERAPEUTIC MODEL IS AND WHY IT IS IMPORTANT TO HAVE ONE - PATRICK TOMLINSON (2019, revised 2026)
Date added: 01/05/24
Download a PDF of this Article
(The PDF at hte bottom of this page is the revised version. There are also 2 PDFs on International Research)
“In Australia, the most clearly articulated model of Therapeutic Residential Care is that offered by the Lighthouse Foundation (Ainsworth 2012; Barton, Gonzales and Tomlinson 2012) that owes much to the Cotswold Community in the UK.” (Thoburn and Ainsworth, 2015, p.45)
Introduction
In recent decades therapeutic models for children and young people, who have suffered trauma and who are in residential or foster care have become more widespread. Working with organizations to develop therapeutic models is one of the main areas of my work. I have done this work for over 20 years in various countries such as UK, Australia, Japan, Ireland, and Portugal. I have developed a workplace curriculum for model development, which is culturally sensitive.
This group of young people have major difficulties, which can cause serious if not disastrous lifelong problems for themselves, others and society. Specialist intervention is needed, and it is often expensive. Therefore, many governments and professionals have been focused on discovering ‘what works’. This article attempts to explain what a therapeutic model is and why it is so important.
As Thoburn and Ainsworth imply above, there are universal elements in therapeutic work with people who have suffered trauma and adversity. The core principles of a therapeutic model tend to be transferable from one setting to another. These are principles such as,
• the centrality of relationships
• a phased approach beginning with safety
• the need to regulate emotion
• and the importance of the whole system.
The value of having a coherent model is in itself a core principle. The principles are informed by research and the best evidence available. However, exactly how these principles are implemented in practice needs to reflect the local culture. There will also be some aspects of a model that are unique to a specific culture. Models must be culturally sensitive. They must be grounded in cultural values, language and belief systems.
This article is specifically relevant to work with children and young people who are in residential care or foster care, throughout the world. However, much of it may also be relevant to other areas of therapeutic work. A therapeutic model in effect is a method of working with human suffering, intending to achieve improvements. Though the language is new, the idea is not. In work with children and young people, models have certainly existed throughout the 20th century. They tended to be created by pioneers, who researched, implemented and passed them on. This was often done by creating a centre/institution/therapeutic community which embodied the model. Sometimes, even when excellent outcomes seemed to be achieved, people outside of these centres understood little about the practice. There was sometimes an air of mysticism. Although, pioneers such as Bruno Bettleheim in the USA, Barbara Dockar-Drysdale in England and John Brown in Canada among others, did write substantially about their work, ideas, and methods.
One of the main differences these days is a growing expectation for a model to be clearly articulated in a written document. This makes it potentially more accessible. It also means that it can be more easily critiqued and challenged. Following on from that there is an expectation that a model should be informed by research and evidence.
However, there are also potential problems with a written model. For instance, the interpretation of it may not be consistent. It may also appear to be like a manual that will provide all the answers. This is always an issue in human services, which tend to involve ‘messiness’, unpredictability and pain. There can be an understandable wish for the order that a ‘manual’ might appear to provide. As Thompson (2000, p.80) argues,
If we expect theory to provide ready-made answers to the questions practice poses, we are misunderstanding not only the nature of theory, but also of practice. Theory cannot provide simple answers which tell us ‘how to do’ practice. Theory can only guide and inform. Theory, practice and the relationship between them are all far too complex for there to be a clear, simple and unambiguous path for practitioners to follow. Theory provides us with the cloth from which to tailor our garment, it does not provide ‘off-the-peg’ solutions to practice problems.
Recovery is a process rather than an event and there is no perfect recovery. Thompson (2000) also talks about the ‘notion of uncertainty, of no security and no guarantees’ as being important for practice. There is not a simple solution to recovery from trauma. It cannot be prescribed but needs an environment where it is safe to think about the trauma, experience feelings about it and make reliable provision to heal it. This type of environment has been referred to as a ’holding environment’. Whilst having our guiding principles and experience we must also keep in mind that every child, worker, situation organization and cultural context is unique.
So, if we are going to have well-articulated models, we need to use them in the right spirit. Not as rigid doctrines, but something with helpful parameters, which provides guidance and supports people in their difficult work. To assist with, rather than replace thinking.
I deliberately use many references in this article, partly to show the depth and consistency of thinking that has emerged across the world. During the last 20 years or so, there has been significant international research into what works in enabling the best outcomes for children (and young people) who are in the ‘Looked-After’ or ‘Out-of-Home’ care system. While it is often said that that we have little ‘evidence’ of what works, it cannot be denied that we do have a vast amount of experience and research to inform us. I think it is important to acknowledge the great value of this.
International Research and Development
This article is based on my own experience and the vast research and experience of authors from the USA, UK, Australia, New Zealand, Ireland, and Canada. The research has examined all past studies and has reached a consistent point of view on the fundamental principles of positive service provision.
During the same period, there have been major advances in neuroscientific research on child development, the impact of trauma and the most effective interventions to facilitate recovery. However, as McHugh and Meenan (2013, p.251) argue, doing this well is a complex challenge,
The needs and problems of many children in care are complex and difficult to serve appropriately. Or more correctly, their needs are deceptively simple, but delivering the right response is deceptively complex (Gilligan, 2001: 1).
Taylor (2012, p.100) highlights the significant work of Clough et al. (2006) who,
…found that a significant factor in successful residential care is a coherent model based on a clear theoretical perspective.
and (ibid, p.3) referring to Fonagy (2006) that,
Traumatized children benefit from the experience of living in a carefully considered, well-structured and coherent psychosocial environment where interpersonal interactions are thought about and reflected on.
Numerous effective therapeutic models have been created during the last two decades. Based on their research into the implementation of different models of care, Macdonald and Millen (2012) recommend,
The introduction of an explicit model of care, championed by the heads of homes and delivered in collaboration with a whole staff team, has much to recommend it in terms of the existing evidence regarding how best to improve the quality of care.
Most importantly a therapeutic model helps improve staffs understanding of children and their needs, so better outcomes can be achieved,
Understanding how children’s responses may have been shaped by maltreatment, including neglect, is thought to help staff respond sensitively and appropriately to challenging or unhelpful behaviour, and to provide opportunities for new, positive experiences that may help to reverse the adverse consequences of early childhood adversity (Cicchetti and Rogosch, 2001; Moses and Barlow, 2006; Gunnar and Quevedo, 2007). (Macdonald and Millen, 2012).
What is a Model?
While most people might not think consciously in terms of models - in essence, they are like John Bowlby’s (1969) concept of internal working models. Bowlby used the term in his work on attachment theory. It may be one of the first uses of the word model in our field of work. It is the way we make sense of the world, our part in it and our purpose. This is true for individuals, organizations, and societies. For instance, what does one want to achieve; what methods will we use; what evidence exists about the effectiveness of the methods; and what are the potential outcomes; including unintended outcomes or side-effects? (Tomlinson, 2014). Macdonald and Millen (2012) put this into the organizational context,
At its core, a theory of change spells out how the core components of an intervention (its ‘inputs’) bring about changes in staff behaviour and organizational processes or culture (the ‘outputs’) and why or how these changes are thought to benefit children and young people (‘outcomes’).
They continue to elaborate on how change takes place,
The implicit theory of change appears to be as follows: by bringing staff to a shared understanding of trauma and its effects, and providing them with a language with which to communicate that understanding, staff can bring about the changes in organizational behaviours, structures and processes needed to address the detrimental effects of trauma.
As Mackay (2014, p.37) states it is vital that the model is adapted to the specific needs of the children involved,
It is important that whatever model is developed it is made to fit the child and not the other way round.
Redshaw (2001, p.16) who has carried out extensive work on model development outlines the following qualities of a model of care.
• It is a well-defined set of procedures and practices
• It is proactive, not reactive
• Increases consistency
• Aids in data collection, evaluation, and reviews of program
A model can provide guiding principles, standards, specific techniques, some do’s and don’ts. But most importantly it should equip the people doing the work with the ability to think within a framework and work things out together. A model provides parameters within which things can be tried and monitored. What works can carry on and what doesn’t may need re-thinking or persevering with. Having a benchmark provides a point from which new ideas can be critiqued. If there isn't a benchmark how do we notice how far something is drifting - a bit like walking in the fog, without even a vague marker to keep a sense of direction.
Aims of a Model
The aim of a model is multi-fold, to provide,
1. Knowledge and understanding so that the children’s needs will be responded to most effectively. This requires the creation of an ethos, which will influence every aspect of the children’s daily life.
2. A consistent and congruent approach in the best interests of the child (Anglin, 2002).
3. Guidance on specific therapeutic interventions, which target specific needs identified through an assessment.
Wall et al. (2013, p10) referring to Redshaw (2011, 2012) claim,
The intention of the model is to provide a body of knowledge and a practice framework to assist in the avoidance of the age old challenge to residential care practice which sees workers fall back on their own personal parenting practices and belief systems and instinctive reactions to young people which are often not helpful; the model seeks to support workers to view the young person from multiple perspectives to allow a holistic approach to intervention and healing.
Evidence-Based Practice
The emergence of therapeutic models has been influenced by the development of evidence-based practice. As Farrelly (2013, p.123) explains,
Evidence-based practice has become a byword for better, more appropriate and efficient practice. In essence, an evidence-based approach asks that practitioners use the best available evidence to guide and inform their practice. There is nothing particularly new about the idea that policy and practice should be informed by the best available evidence/Evidence-based practice (EBP) was first introduced in medicine and allied health professions. More recently it has been advocated in social work as an alternative to 'authority-based practice' or practice based solely on the expertise and experience of practitioners (Edmond et al., 2006) …EBP represents a move away from opinion, past practice and precedent and towards a decision-making framework that relies on greater use of research and evidence.
Evidence from practice becomes part of the knowledge that underpins social care. Knowledge = evidence + practice wisdom + service user and carer experiences and wishes. All three elements are equal in contributing to knowledge. Therefore researchers, practitioners and service users all have an equally valid role in contributing to knowledge (Farrelly, 2013, p.131). A model will influence practice and practice will influence the model. This leads to the concept of the ‘research-minded practitioner’ (ibid, p.132).
 In my early twenties, I began work at the Cotswold Community, a renowned therapeutic community in England. The Community began in 1967 and I started work there in 1985. The development of its model, though the term model was not used then, had involved leading experts in the field. By the time I arrived, the Community had student placements and visitors from all over the world. I had virtually no relevant work experience. However, I was struck from the beginning by how we were encouraged to reflect upon our experiences and make contributions that might further develop the model. We adopted the same approach in the way we tried to listen to and learn from the children. Connected with this philosophy, McHugh and Meenan (2013, p.258) argue that the challenge is.
In my early twenties, I began work at the Cotswold Community, a renowned therapeutic community in England. The Community began in 1967 and I started work there in 1985. The development of its model, though the term model was not used then, had involved leading experts in the field. By the time I arrived, the Community had student placements and visitors from all over the world. I had virtually no relevant work experience. However, I was struck from the beginning by how we were encouraged to reflect upon our experiences and make contributions that might further develop the model. We adopted the same approach in the way we tried to listen to and learn from the children. Connected with this philosophy, McHugh and Meenan (2013, p.258) argue that the challenge is.
To move from learning about to learning with children in care.
Farrelly (p.124) adds a cautionary note,
While the arguments for the adoption of an evidence-based approach may be convincing, it should be noted that finding and using research, particularly of high relevance and good quality, is not always easy.
It is exceedingly difficult to have what would usually be called scientific evidence, in such a complex field of work with so many variables.
Research-Informed
As said earlier, a therapeutic model must be informed by research and the best knowledge available. Referring to social care guidelines in Ireland, Farrelly (2013, p.123) states the importance of practice being informed by research,
The Department of Health and Children's (DoHC) policy document Working for Children and Families: Exploring Good Practice outlines seven management principles that should underpin child and family services, including the need for practitioners and their managers to 'ensure that their practice and its supervision are grounded in the most up-to-date knowledge' (2004: 15). More recently, the Health Information and Quality Authority's (HIQA) National Standards for the Protection and Welfare of Children state that standards need to be person-centred and 'based on evidence and best international practice’ (2012: iii).
Farrelly (2013, p.133-4) argues that the amount of the ‘research that constitutes 'quality evidence' remains debatable’ and warns of adopting a too dogmatic approach to evidence-based practice,
Social services are by their very nature fluid and dynamic, and practitioners need to be mindful of the potential to adopt a dogmatic approach. Sheppard (2004: 23) argues that practitioners should be 'looking at information that can help provide guidance and better informed judgements but not certainty'. Perhaps, given the nature of the debate and the nature of the work that the social professions are engaged in, the term 'research-informed practice' might be more applicable than 'evidence-based practice'.
Institute of Child Protection Studies (2006, p.12) in Australia refers to the research of the last 20 years and particularly that of Clough et al. (2006). They highlight some of the universal principles of a model,
Whilst the literature review has not identified a specific model that is easily replicated it has identified the important elements for providing such care. These elements include,
• the creation of a clear ethos and positive culture
• individualised assessment and planning
• collaborative practices
• the involvement of family members
• the involvement of young people in planning and decision making
• positive peer relationships
• a coherent theoretical framework with the identification of values, objectives of the programme, theories of behaviour, of intervention and of organization
• developing resilience through education, learning and leisure interests
In particular, the maximising of the day to day and opportunity led communication and connection to promote healing relationships seems to lie at the heart of effective residential care.
Brandt (2014, p.11) states the importance of a therapeutic research-informed model,
Ideally, ther¬apeutic work is derived from and grounded in theoretical constructs, research evidence, and the logical construction of strategies or approaches where work is improvisational and contextual—and optimally this process is guided by an explicit therapeutic model.
Kezelman and Stavropoulos (2012, p.xxviii) in their work on creating trauma-informed services affirm the necessity of research.
Research shows that the impacts of even severe early trauma can be resolved, and its negative intergenerational effects can be intercepted. People can and do recover and their children can do well. For this to occur, mental health and human service delivery need to reflect the current research insights.
Key Elements of a Model
Irrespective of which theories inform residential care practice, it has been argued that effective residential care needs to incorporate:
(a) a clearly thought-out philosophy of treatment or care (Clough, 2008; Hillan, 2006, Sinclair and Gibbs, 1998);
(b) child-centred practice, in which service provision is matched and responsive to the child’s need, rather than the child’s needs being subordinate to the service model (Clough, 2008; Hillan, 2006);
(c) a service-wide commitment to staff support and continuous learning (Hillan, 2006).
McLean et al. (2011, p.11).
Institute of Child Protection Studies (2006, p.31) in Australia state,
James Anglin (1999, p.144) has written about the distinctive nature of what he calls the ‘child and youth care profession’ which he says has five characteristics,
• a focus on the growth and development of children and youth
• concern with totality of a young person’s functioning, rather than one part of functioning
• ‘a social competence perspective’, which builds on strengths, rather than a problem-based approach
• direct day-to-day work with children and young people in their environment, rather than being restricted to interviews or sessions
• the development of therapeutic relationships with children, their families and other helpers.
Whole-System Approach
 Clough et al. (2006) found through their research into what works in residential care, that positive outcomes for children are linked to a strong children's culture, which in turn is linked to a strong staff culture. This finding is supported by Warner (1992) who found that positive outcomes were only correlated with leadership and clarity of purpose. Therefore, it is important that a therapeutic model considers the whole system and not just the direct work with children.
Clough et al. (2006) found through their research into what works in residential care, that positive outcomes for children are linked to a strong children's culture, which in turn is linked to a strong staff culture. This finding is supported by Warner (1992) who found that positive outcomes were only correlated with leadership and clarity of purpose. Therefore, it is important that a therapeutic model considers the whole system and not just the direct work with children.
A whole-system model is one that spans across all aspects of the child’s daily living situation. It requires that the relationships between the different parts involved are fully integrated into the model. Childhood trauma takes place in an environment - trauma is in the system, not the event. Cissy White (2018) explains this very well,
Being raised with ACEs (adverse childhood experiences) is an environment, not a series of incidents that happened here and there. I lived every day with scarcity and lack. Trauma was baked into my being, as were my responses.
Similarly, therapeutic work also takes place in an environment with a network of relationships. As Macdonald and Millen (2012) state,
Models articulate the inter-relationships of their component parts and the pathways of change embedded within them.
Kezelman and Stavropoulos (2012, p.xxx) link the organizational context and the recovery process,
 “Research now shows that resolution of trauma equates with neural integration. It also shows that longstanding trauma can be resolved, and its negative intergenerational effects intercepted. But for this to occur, mental health and human service delivery (i.e. as well as direct treatments) need to reflect the current research insights. Experience is now known to impact brain structure and functioning, and in the relational context of healing this includes experience of services. Neural integration is not assisted – indeed is actively impeded – by unintegrated human services which are not only compartmentalised, but which lack basic trauma awareness.”
“Research now shows that resolution of trauma equates with neural integration. It also shows that longstanding trauma can be resolved, and its negative intergenerational effects intercepted. But for this to occur, mental health and human service delivery (i.e. as well as direct treatments) need to reflect the current research insights. Experience is now known to impact brain structure and functioning, and in the relational context of healing this includes experience of services. Neural integration is not assisted – indeed is actively impeded – by unintegrated human services which are not only compartmentalised, but which lack basic trauma awareness.”
They (p.16) emphasize the importance of the ‘whole-system’ approach,
"Both administrative and clinical experience suggests that attributes of the system `as a whole’ have a very significant impact on the implementation and potentially the effectiveness of any services offered."
Whole-system models focus on providing training to all staff within the organization, whatever their role. In one organization I worked with, trauma-informed training was given to the whole workforce. This included care workers, managers, therapists, admin workers, human resources, finance and maintenance. The effect of this training, which everyone did together contributed to a cultural transformation. Not only did the training enable staff to be better trauma-informed, but the way it was done was inclusive, brought people together, helped to build connections, and gave everyone a shared understanding of the organization’s primary task.
Importance of a Theoretical Base
UK’s Social Care Institute of Excellence (2012) in their research into different models, highlight the helpfulness of having a theoretical base,
Staff who can think clearly and logically about their work use a set of strategies to understand children’s behaviour and critically evaluate their own actions and those of others and use their understanding to act in the best interests of children are likely to be better at their job than those who have no framework.
There is a long tradition of specialized therapeutic services for children having a strong theoretical base. Fahlberg (1990, 51) emphasized the importance of a theoretical base to residential treatment,
The most important task of treatment must be clearly and succinctly stated. Specific problems and dynamics vary from child to child, but a philosophy of treatment must clearly identify the category of problems that are most essential for the programme to confront if successful treatment is to occur.
In more recent times, the field of neuroscience has become a central part of the theory as Perry (2014, p.30) explains,
A developmentally sensitive and neurobiology-informed clinical approach can aid the clinical team in understanding the impact of maltreatment and other devel¬opmental insults.
Stien and Kendall (2004, p.7) claim that the new neurobiology represents a confluence of two strands of brain research – attachment theory and childhood trauma,
Whereas traumatologists focus on abnormal development, attachment researchers often examine the brain under conditions of normal or optimal development. Thus, when taken together, these two strands of research clarify the key mechanisms behind both mental health and psychopathology in chil¬dren. Whereas secure attachment produces a growth-facilitating envi¬ronment that builds neuronal connections and integrates brain systems, strengthening the capacity to cope with stress; abuse and neglect in¬duces chaotic biochemical changes that interfere in the maturation of the brain's coping systems, leading to problems with emotional regula-tion, relationships, and identity formation (Schore, 2001).
Historically John Bowlby and Donald Winnicott had a huge influence on the development of therapeutic approaches, as outlined by Byrne (2013, p.143),
 "Possibly the most influential psychodynamic theorists within therapeutic social care are Donald Winnicott and John Bowlby. Winnicott's work with therapeutic communities in Britain is the primary influence for contemporary theorists in this area such as Adrian Ward (Ward et al., 2003). There probably is no social care practitioner in Ireland whose practice has not been influenced by John Bowlby's attachment theory (see, for example, Fahlberg, 1994)."
"Possibly the most influential psychodynamic theorists within therapeutic social care are Donald Winnicott and John Bowlby. Winnicott's work with therapeutic communities in Britain is the primary influence for contemporary theorists in this area such as Adrian Ward (Ward et al., 2003). There probably is no social care practitioner in Ireland whose practice has not been influenced by John Bowlby's attachment theory (see, for example, Fahlberg, 1994)."
The leading neuroscientist Bessel van der Kolk (2014) referring to attunement which is a vital concept in neuroscience claims that,
"Donald Winnicott is the father of modern studies of attunement."
Macdonald and Millen (2012) argue that a theoretical base can help services to be effective,
"The importance of theory informed therapeutic care and the centrality of relationship- based social work were also found to be essential in promoting resilience within the young people."
Fosha (2003, p.276) claims that the challenge is to operationalize the substantial evidence base of affective neuroscience into a `neurobiology of healing’.
Macdonald and Millen (2012) in their review of different models say that,
Each provides a framework whose constituent theories are intended to help staff to understand:
• How trauma impacts on children and young people.
• How and why their ways of coping might be maladaptive.
• How and why agencies and staff respond in ways that are not always helpful.
• How they might change. Each emphasises the importance of helping staff develop the knowledge and skills necessary to help those they care for.
Without a theoretical base, it is difficult for staff to be trained to a level that enables them to provide consistent, coherent and appropriate care.
Different Theoretical Perspectives
Mackay (2014, p.22) explains the need for approaches informed by different perspectives,
The growing body of knowledge in the areas of attachment, trauma and neurodevelopment tells us that it takes multiple therapeutic interventions on a daily basis to effect permanent and lasting change for these young people. These interventions are most effective when carried out by people with whom the young person has a relationship (Boyd, et al., 2013; Burnside 2012; Child Protection Development Department of Communities 2011; Cook et al., 2005; McClung 2007; Perry 2009; Prasad 2011; van der Kolk 2005).
Kezelman and Stavropoulos (2012, p.76) also argue the benefit of drawing knowledge from different theoretical perspectives,
While effective treatment of complex trauma needs to address several key dimensions (i.e. irrespective of the particular approach used) the current literature also advises of the need for knowledge of more than one modality.
Many theories may be useful for different aspects of the therapeutic task. Theoretical knowledge from the following fields are essential in all therapeutic residential services for children,
- Child Development
- Attachment
- Neuroscience
- Trauma
- Loss and Grief
- Psychodynamic
- Systems
Training
Only when there is a coherent model is it possible to design appropriately focused training. The Department of Communities (2010, p.13) highlight the importance of staff training,
International research also speaks to the need for well-trained staff and notes that one of the most negative factors influencing poor outcomes for young people is untrained staff. According to expert Jim Anglin, it is ‘a disturbing fact that those who have the most complex and demanding role in the care and treatment of traumatised children have the least, and in many cases, no specific training for the work’ (Anglin 2002b, p113). Acknowledgement of the need for enhanced training for residential staff is increasing both nationally and internationally.
McHugh and Meenan (2013, p.250) make a similar point,
Professional training provides opportunities to develop and practise skills and heighten self-awareness. These opportunities, coupled with relevant theory, promote a reflective approach to social care practice. It is the responsibility of the individual practitioner and of the service provider to ensure that all staff are both aware of and equipped for their professional role.
Furnivall et al. (2012, p.49) state,
For all practitioners, however, it is crucial that training is delivered by people who understand the context in which their practice takes place and in a manner which is congruent with an attachment-informed approach.
The emphasis of training should be on improving everyone’s understanding of the children, how their development has been impacted by trauma and what approaches are most likely to help. In her paper, The Importance of Child Care Training, Barbara Kahan (1995, p.1) argues that we would expect lawyers, dentists, doctors and teachers to be trained, qualified and up-to-date with recent knowledge,
…so why are we prepared to tolerate a situation in which, by definition, some of the most needy and traumatized children in our community are cared for by people who, however well-intentioned, are neither trained, qualified nor, in many instances, knowledgeable about their needs and how best to deal with them?
Having a Model is the Most Important Thing
Whilst many different models have been created the underlying principles tend to be remarkably similar. The research is consistent on the importance of key matters, such as,
• relationships
• attachment
• attunement
• meeting emotional needs
• consistency of teamwork
• whole-system approach, etc.
It can be argued that as long as a model is based on these key parameters, it is the coherency and consistency that it brings that is most important. Macdonald and Millen (2012) state,
There may be merit in the argument that it is providing staff with “a framework? within which to think about their work that matters, rather than a particular framework. Staff who can think analytically about their work, who can better understand children’s behaviour and critically appraise their own actions and those of others, and who can draw on their understanding to act in the best interests of children, are likely to be better at their job than those who have no such framework. They are also likely to have more job satisfaction and, particularly when whole staff teams are trained in that framework, more likely to behave consistently – something we know children value.
Janet Rich, (2009) strongly supports this view,
It is almost certainly the case that the specific model of care adopted is far less important than the fact of there being a model of care that is underpinned by an empirical and theoretical evidence base, that the staff and young people are signed up to, and that is supported by both an established culture within the home, by sound leadership and supervision structures and by appropriate training and resources.
Like parenting, what helps children develop, is as much to do with the quality of relationships between the carers, and the nurturing and predictable environment provided – rather than the exact detail of the approach and personality type of the carer. It is helpful if parents have similar models of what children need. Byrne (2013, p.146) agrees with the view that a coherent model improves the consistency of practice,
When practitioners identify themselves as providing therapeutic care it is important that they are clear about the approach that informs their practice. The reason is that where several practitioners are working with the same client, the active interventions will be different depending on the theory influencing each individual practitioner. Mixed approaches could lead to inconsistency in service provision and unhelpful or confusing outcomes for the client.
McLean et al. (2011, p.13) explain the value of a model to the professionals involved,
From a service perspective, providing staff members with a coherent strategy and conceptual framework for understanding and addressing challenging behaviour, as well as a strategy to manage risk and de-escalate behaviour during critical incidents, while also maintaining their relationships with children in the unit, is likely to be valued.
The best knowledge available provides a guiding framework, within which to think about children’s needs. Macdonald et al. (2012, p.14) expands upon the benefits for professionals of having a guiding framework,
There is value in the argument that the principal value of a model lies in giving staff a coherent “conceptual framework? to think about the work that matters. After all, staff who can: think clearly and logically about their work use a set of strategies to understand children’s behaviour and critically evaluate their own actions and those of others use their understanding to act in the best interests of children are likely to be better at their job than those who have no framework……..They are also likely to have more job satisfaction and – particularly when whole staff teams are trained in that framework – likely to behave consistently, which is something we know that children value.
‘Import’ or Create a Model?
As mentioned, many different models have been created in recent times. Although there are differences most models also have much in common. This raises the question of whether to adopt an ‘off-the-shelf’ model or create a unique local model. The former may have a stronger evidence-base, being tried and tested. The latter may achieve greater staff engagement and be more culturally sensitive. Having ownership can also make a big difference. The model belongs to the organization. This helps improve a sense of security which is especially important in a field of work, which has so much uncertainty and vulnerability. Ownership is so important that one organization I worked with made it one of their core values.
I am sure that both approaches can work well. My own experience is in developing models that are unique but based on key research-informed principles. I find that this leads to a high level of engagement, creativity, and ownership. These models have achieved excellent outcomes and wide acclaim. However, having a good model on paper is not a guarantee of good outcomes. Other vitally important factors will also determine success. For example,
• the quality of leadership
• is the model embedded in the culture?
• is it understood?
• and do people feel a sense of ownership?
It is the combination of all such factors along with the model that determines the quality of outcomes. In some cases, an organization may have already developed a model over many years – but has not fully articulated it. In this case, the task may be more to do with,
• reviewing the model
• writing it up
• and underpinning with research-informed theory.
Continual Evolution
Once we have a model, we must ensure it continues to evolve. Models must be alive and adaptive. They must be open systems and have feedback loops, so they can receive the information they need from all parts of the system. They must learn and develop from direct experience and wider research. In other words, a model can never become a fixed entity. As one part of the system changes other parts must adapt. Continuous evolution is essential.
For example, a change in the external environment, politically, economically, or professionally will require an adaptation. As with evolution, those that are most adaptive are most likely to survive. In one organization I worked in that had a strong model, we also had a working group every week to reflect upon, clarify our practice and suggest ideas for improvement. This was then fed back to the wider organization for further consideration. Just like organizations, a model is a living system.
Outcomes
 Willis (2001, p.139) referring to the UK Department of Health initiatives of the 1990s, states the centrality of outcomes,
Willis (2001, p.139) referring to the UK Department of Health initiatives of the 1990s, states the centrality of outcomes,
“Social care services are likely to be most effective when they are orientated towards outcomes: concerned with, designed, provided and evaluated in terms of the results experienced by the people for whom they are intended (SSI, 1993, p.9).”
The concept that services should be based on ‘children’s best interests’ has become a touchstone for child and youth care practice (Anglin, 2004, p.177). We need to have a general idea of what the ‘children’s best interests’ are. This clarifies the outcomes that we aim to achieve for each child. An outcomes-focused approach has a clear intent to deliver positive outcomes that can be evidenced. As Department for Child Protection (2009, p.3) put it,
In a therapeutic situation, it is essential that children and young people and the care workers understand what they want to achieve, so that their goals and strategies for achieving those goals are aligned.
Or as The Department of Health (1998) succinctly stated,
There is a need for clearly stated objectives of what the residential care unit wishes to achieve. (In, Institute of Child Protection Studies, 2006, p.20).
Kezelman and Stavropoulos (2012, p.81) argue that given that complex childhood trauma continues to be inadequately defined and covered by standard interventions, it is important to focus on the outcomes rather than a ‘one size fits all’ treatment. To know what outcomes are being achieved or not there must be a reliable and appropriate form of assessment. Assessments need to focus on the most important outcomes and areas of development. For example, how a child can learn, manage emotions and make healthy relationships. Ward (2004) makes two particularly important points about assessment,
1. You can have assessment without treatment, but you certainly can’t have treatment without assessment.
2. What matters most... is that the whole team is engaged both in the process of assessment and in the process of treatment.
Overarching Outcomes and Benefits of Having a Model
1. A clearly articulated model clarifies the task and reduces confusion. This leads to a higher level of congruence, with improved outcomes for all stakeholders.
2. A model creates a shared language and processes, which helps integrate different professional disciplines.
3. It is highly beneficial for organizations to understand trauma and how to respond to it. This is becoming trauma-Informed.
4. Greater consistency and quality of professional and organizational development. Improved performance, funding and cost-efficiency.
5. The development work is a helpful way of reviewing the organization’s culture and practice.
6. The work involved will be a positive experience of team building - creating a shared vision, values, and commitment. The involvement of the organization in the creation process will lead to a high level of engagement and ownership.
7. A high-quality model will further consolidate the organization’s position – in terms of being a high caliber service provider, attracting referrals, funding and good quality staff.
8. Holding a conference, publishing papers/a book all help to establish the organization as a leading authority in the field.
9. In some countries having an articulated therapeutic model is becoming a Government requirement, influencing the placement of children. Therefore, not having a model could jeopardize an organization’s future.
Long-term and Societal Impact
As well as benefits to the young people, the organization and all those directly involved, there will also be significant benefits to society. The life-long prospects for the children’s well-being should be greatly improved. They are more likely to grow up into healthy adults, making a positive contribution to society.
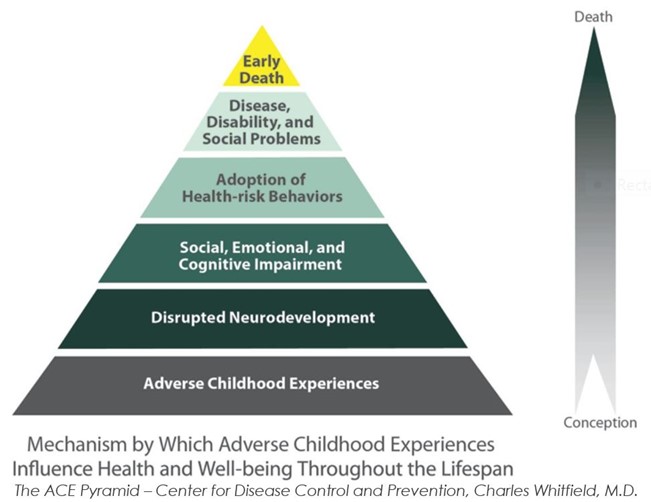 Whereas children who are in care and who do not experience an effective service are more likely to have serious difficulties as adults, becoming a burden on society. This is likely to be seen in areas, such as poor health and early death, drug and alcohol addiction, mental health problems, abusive behaviour, and criminal activity. The ACEs study has made truly clear the potential long-term consequences of Adverse Childhood Experiences, especially when there is no positive intervention (AAP, 2014).
Whereas children who are in care and who do not experience an effective service are more likely to have serious difficulties as adults, becoming a burden on society. This is likely to be seen in areas, such as poor health and early death, drug and alcohol addiction, mental health problems, abusive behaviour, and criminal activity. The ACEs study has made truly clear the potential long-term consequences of Adverse Childhood Experiences, especially when there is no positive intervention (AAP, 2014).
Hannon et al. (2010, p.162) illustrate this well in the graph below, from their research paper.
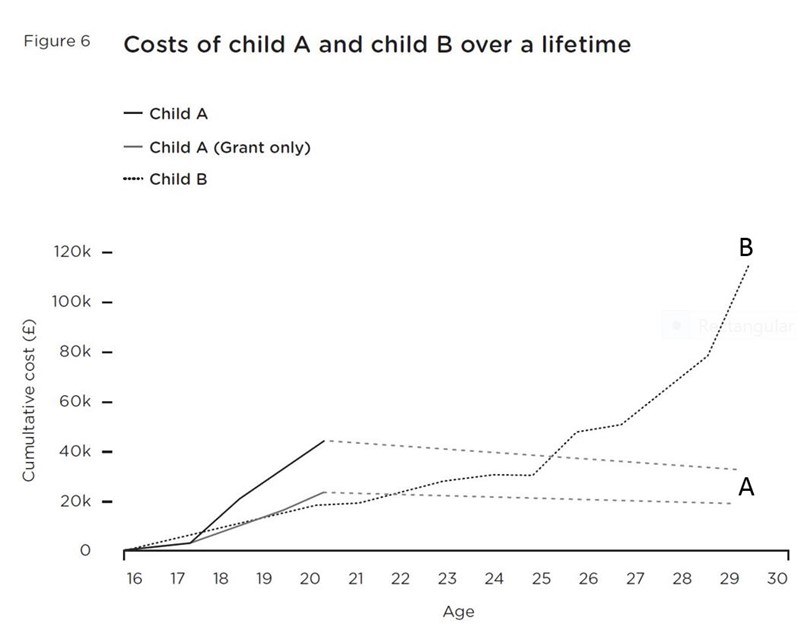 This graph compares the costs of care for child A and B. Child B has a poor experience in ‘out of home’ care. The costs associated with this child continue to escalate from the age of 16-30 and will continue over a lifetime. Child A has a positive experience of high-quality care. Initially, the costs for Child A are higher than for Child B. However, by the age of 21, the cumulative cost is reducing and will continue over a lifetime. The higher of the two Child A lines include student loan costs. The lower Child A line is without loan costs as they can be expected to be paid back over a lifetime. The initial higher cost for Child A is paid back over time as he/she begins to make a positive contribution to society, through employment and taxes, etc.
This graph compares the costs of care for child A and B. Child B has a poor experience in ‘out of home’ care. The costs associated with this child continue to escalate from the age of 16-30 and will continue over a lifetime. Child A has a positive experience of high-quality care. Initially, the costs for Child A are higher than for Child B. However, by the age of 21, the cumulative cost is reducing and will continue over a lifetime. The higher of the two Child A lines include student loan costs. The lower Child A line is without loan costs as they can be expected to be paid back over a lifetime. The initial higher cost for Child A is paid back over time as he/she begins to make a positive contribution to society, through employment and taxes, etc.
This research was carried out in 2010 and the actual cost numbers in £ are not so relevant. What is relevant and applicable to any country today is the trend. Costs of a good quality service with a therapeutic model will be more expensive in the short term. However, in the medium term and over a lifetime, the financial cost is removed. Whereas the financial cost of Child B continues to escalate, along with the human cost and burden to society. This graph only shows until the age of 30, but it is clear how the trend will continue over a lifetime. As we know, deprivation and abuse tend to continue in cycles, therefore the costs may well continue into further generations. The cost-effectiveness on human and financial levels, of investing in the higher quality service is almost immeasurable.
The Lighthouse Foundation in Melbourne, Australia is one such example. I worked with them on the development of their Therapeutic Family Model of Care™,
Recently an independent assessment was commissioned by Social Ventures Australia to complete an analysis of Lighthouse Foundation’s Social Return on Investment (SROI). It proved for every dollar received Lighthouse returns $12 of social value. (Lighthouse Foundation, 2019)
Process of Change, Model Development, and Implementation
This article has attempted to explain what a therapeutic model is and why it is important. It has implied the work that is involved but not discussed the process of development and implementation, which is a whole subject. The development process is fundamentally one of significant organizational change. It will be greatly valuable, but also challenging and difficult. There will need to be processes such as supervision, training and consultation to work through the issues involved. Some of this work will take place before the model development begins and it can continue alongside. Without this work, there is a greater risk that the development project will be undermined.
Model development must take place alongside processes that look at and work on the issues of change. The importance of strong leadership cannot be underestimated. An organization that has developed a positive and effective way of working, will need time to take that to the next stage and clearly define their model. In my experience, a rough guideline would be around one year to articulate the model and write it down, another year to implement it, and a further year to establish it. The actual timelines will be influenced by the organization’s stage of development, the level of resources committed to the project and whatever challenges arise along the way. When a model is achieved the potential benefits that I have outlined are great. Bringing people together to work on such a key shared task can also have many benefits.
Given the immense challenges in this work, as van der Kolk and McFarlane (2007, p.574) have claimed,
This struggle to transcend the effects of trauma is among the noblest aspects of human history.
References and Further Reading
AAP (2014) Adverse Childhood Experiences and the Lifelong Consequences of Trauma, American Academy of Pediatrics, accessed February 8th, 2019, https://www.aap.org/en-us/Documents/ttb_aces_consequences.pdf
Ainsworth, F. (2012) ‘Therapeutic Residential Care for Children and Young People: An Attachment and Trauma-Informed Model for Practice.’ Book Review, in Children Australia, 37, 2, 80
Anglin, J. (1999) The Uniqueness of Child and Youth Care: A Personal Perspective, in Child and Youth Care Forum, 28(2), 143-150
Anglin, J. (2002) Pain, Normality, and the Struggle for Congruence: Reinterpreting Residential Care for Children and Youth, New York: The Haworth Press Inc.
Anglin, J. (2002b) Risk, Well-being and Paramountcy in Child Protection: The Need for Transformation, Child and Youth Care Forum, vol. 31, no. 4, 257-268
Anglin, J. P. (2004) Creating “Well-Functioning” Residential Care and Defining Its Place in a System of Care, in Child and Youth Care Forum, 33 (3), June 2004, Canada: Human Services Press, Inc.
Barton, S., Gonzalez, R. and Tomlinson, P. (2012) Therapeutic Residential Care for Children and Young People: An Attachment and Trauma-informed Model for Practice, London and Philadelphia: Jessica Kingsley Publishers
Bowlby, J. (1969) Attachment. Attachment and loss: Vol. 1. Loss, New York: Basic Books
Boyd, L. W., Brylske, P. and Wall, E. (2013) Beyond Safety and Permanency: Promoting Social and Emotional Well-Being for Youth in Treatment Foster Care, Foster Family-based Treatment Association
Brandt, K. (2014) Core Concepts in Infant-Family and Early Childhood Mental Health, in Brandt, K., Perry, B.D., Seligman, S. and Tronick, E. Infant and Early Childhood Mental Health: Core Concepts and Clinical Practice, Washington D.C. and London: American Psychiatric Publishing
Byrne, J. (2013) Therapeutic social care practice, in Lalor, K. and Share, P. (Eds.) (2013) Applied Social Care: An Introduction for Students in Ireland, Dublin: Gill and Macmillan
Burnside, L. (2012) Youth in Care with Complex Needs, Manitoba Office of the Children's Advocate
Child Protection Development Department of Communities (2011) Specialist Foster Care Review: Enhanced Foster Care Literature Review and Australian Programs Description, Queensland: Department of Communities
Cicchetti, D., and Rogosch, F. A. (2001) The impact of Child Maltreatment and Psychopathology upon Neuroendocrine Functioning, in Development and Psychopathology, 13, p.783-804
Clough, R. (2008) A Vision for Residential Care, in Children Australia, 33(2), 39–40
Clough, R., Bullock, R., and Ward, A. (2006) What Works in Residential Child Care: A Review of Research Evidence and the Practical Considerations, London: National Children’s Bureau
Department for Child Protection (2009) Residential Care Conceptual and Operational Framework, East Perth, Australia: Department for Child Protection
Cook, A., Spinazzola, J., Ford, J., Lanktree, C., Blaustein, M., Cloitre, M. and van der Kolk, B. (2005) Complex Trauma in Children and Adolescents, Psychiatric Annals, 35(5), p.390-398
Department of Communities (Child Safety Services) in Partnership with PeakCare Queensland (2010) A Contemporary Model of Residential Care for Children and Young People, Queensland: Queensland: Government
Department of Health (1998) Caring for Children Away from Home: Messages from Research, Chichester: John Wiley and Sons
DoHC (2004) Working for Children and Families: Exploring Good Practice, Dublin: Stationary Office
Edmond, T., Megivern, D., Williams, C., Rochman, E. and Howard, M. (2006) Integrating Evidence-Based Practice and Social Work Field Education, in Journal of Social Work Education, 42(2), p.277-396
Fahlberg, V. (editor) (1990) Residential Treatment, Indianapolis: Perspective Press
Fahlberg, V. (1994) A Child’s Journey through Placement, London: British Association for Adoption and Fostering
Farrelly, T. (2013) Evidence Based Practice in Social Care, in Lalor, K. and Share, P. (Eds.) (2013) Applied Social Care: An Introduction for Students in Ireland, Dublin: Gill and Macmillan
Fonagy, P. (2006) The Mentalization Approach to Social Development, in Allen, J.G. and Fonagy, P. (Eds.) Handbook of Mentalization-Based Treatment, Chichester: John Wiley and Sons
Fosha, D. (2003) Dyadic Regulation and Experiential Work with Emotion and Relatedness in Trauma and Disorganized Attachment, in, Solomon, M.F. and Siegel, D. (Eds.) Healing Trauma: Attachment, Trauma, the Brain, and the Mind, Pp. 221-281. New York: Norton. Web version
Furnivall, J., McKenna, M., McFarlane, S. and Grant, E. (2012) Attachment Matters for All – An Attachment Mapping Exercise for Children's Services in Scotland, Centre for Excellence for Looked After Children in Scotland: Scottish Attachment in Action, www.celcis.org/media/resources/publications/Attachment-Matters-For-All.pdf
Gunnar, M., and Quevedo, K. (2007) The Neurobiology of Stress and Development, in Annual Review of Psychology, 58, 145-173
Hannon, C., Wood, C., and Bazelgate, L. (2010) In Loco Parentis: “To Deliver the Best for Looked After Children, the State must be a Confident Parent…”, London: Demos
Hillan. L. (2006) Churchill Fellow Report. Reclaiming Residential Care – A Positive Choice for Children and Young People in Care
Institute of Child Protection Studies (2006) What Works in Residential Care: literature Review for Marist Care Group, Draft, Australia Catholic University – accessed February 2013,
www.acu.edu.au/__data/assets/pdf_file/0007/53962/WHAT_WORKS_IN_RESIDENTIAL_CARE_for_MYC_2209.pdf
Kahan, B. (1995) The Importance of Child Care Training, Paper Presented at ARCC Conference 12th July 1995
Kezelman, C. and Stavropoulos, P. (2012) The Last Frontier: Practice Guidelines for Treatment of Complex Trauma and Trauma Informed Care and Service Delivery, Australia: Adults Surviving Child Abuse (ASCA)
Lighthouse Foundation, accessed on 8th February 2019
http://lighthousefoundation.org.au/our-work/therapeutic-family-model-of-care/
Macdonald, G. and Millen, S. (2012) Therapeutic Approaches to Social Work in Residential Child Care Settings: Literature Review, SCIE (Social Care Institute of Excellence): Institute of Child Care Research, Queens University Belfast
Macdonald, G., Millen, S., McCann, M., Roscoe, H. and Ewart-Boyle, S. (2012) Children’s and Families’ Services Report 58: Therapeutic Approaches to Social Work in Residential Child Care Settings, SCIE (Social Care Institute of Excellence): Institute of Child Care Research, Queens University Belfast
Mackay, R. (2014) Creating Successful Outcomes for Youth in Care with Complex Needs and Those who Care for Them, Vodafone New Zealand Foundation
McHugh, J. and Meenan, D. (2013) Residential Child Care, in Lalor, K. and Share, P. (Eds.) (2013) Applied Social Care: An Introduction for Students in Ireland, Dublin: Gill and Macmillan
McLean, S., Price-Robertson, R. and Robinson, E. (2011) Therapeutic Residential Care in Australia: Taking Stock and Looking Forward, Australian Institute of Family Studies: National Child Protection Clearinghouse
McClung, L. F. (2007) Therapeutic Foster Care: Integrating Mental Health and Child Welfare to Provide Care for Traumatised Children: A Literature Overview, Victoria: Berry Street
Moses, E.B. and Barlow, D.H. (2006) A New, Unified Treatment Approach for Emotional Disorders Based on Emotion Science, in Current Directions in Psychological Science, 15, 146-150
Perry, B. D. (2009). Examining Child Maltreatment through a Neurodevelopmental Lens: Clinical Applications of the Neurosequential Model of Therapeutics, in Journal of Loss and Trauma, 14(4), p.240-255
Perry, B.D. (2014) The Neurosequential Model of Therapeutics: Application of a Developmentally Sensitive and Neurobiology-Informed Approach to Clinical Problem Solving in Maltreated Children, in Brandt, K., Perry, B.D., Seligman, S. and Tronick, E. Infant and Early Childhood Mental Health: Core Concepts and Clinical Practice, Washington D.C. and London: American Psychiatric Publishing
Prasad, N. (2011) Using a Neurodevelopmental Lens when Working with Children who have Experienced Maltreatment: A Review of the Literature of Bruce D. Perry, NSW: Uniting Care Children, Young People and Families
Redshaw, S. (2001) Building Blocks for a Quality Care Framework: An Information and Discussion Paper for Mercy Family Services Out-of-Home Care Programs, Australia: Mercy Family Services
Rich, J. (2009) Labels that disable – meeting the complex needs of children in residential care, NICE (National Institute for Health and Care Excellence), www.nice.org.uk/guidance/ph28/evidence/looked-after-children-ep14-labels-that-disable-meeting-the-complex-needs-of-children-in-residential-care-janet-rich2
Schore, A.N. (2001) The Effects of Early Relational Trauma on Right Brain Development, Affect Regulation and Infant Mental Health, in (Electronic Version, p.1-80) Infant Mental Health Journal, 22, 201-269, Retrieved October, 28, 2001, www.trauma-pages.com/schore-2001b.htm
Sheppard, M. (2004) Appraising and Using Social Research in the Human Services: An Introduction for Social Work and Health Professionals, London: Jessica Kingsley
Sinclair, I. and Gibbs, I. (1998) Children’s Homes: A Study in Diversity, Chichester: John Wiley and Sons
Social Care Institute for Excellence (2012) Report 58: Therapeutic Approaches to Social Work in Residential Child Care Settings, www.scie.org.uk/publications/reports/report58/ [Accessed 07/02/2017]
Stien, P.T. and Kendall, J. (2004) Psychological Trauma and the Developing Brain: Neurologically Based Interventions for Troubled Children, New York, London, Oxford: The Haworth Maltreatment and Trauma Press
Taylor, C. (2012) Empathic Care for Children with Disorganized Attachments: A Model for Mentalizing, Attachment and Trauma-Informed Care, London and Philadelphia: Jessica Kingsley Publishers
Thoburn, J. and Ainsworth, F. (2015) Making Sense of Differential Placement Rates for Therapeutic Residential Care: Some Takeaway Messages for Policy, in, Whittaker, J.K., del Valle, J.F. and Holmes, L. (2015) Therapeutic Residential Care for Children: Developing Evidence-Based International Practice, London and Philadelphia: Jessica Kingsley Publishers
Thompson, N. (2000) – Theory and Practice in Human Services, Maidenhead: Open University Press
Tomlinson, P. (2004) Therapeutic Approaches in Work with Traumatized Children and Young People: Theory and Practice, London and Philadelphia: Jessica Kingsley Publishers
Tomlinson, P. (2014) Models in Therapeutic Work with Traumatized Children – Part 1
https://www.patricktomlinson.com/models-in-therapeutic-work-with-traumatized-children-part-1-patrick-tomlinson-2014/18
Tomlinson, P. (2014) Models in Therapeutic Work with Traumatized Children – Part 2
https://www.patricktomlinson.com/models-in-therapeutic-work-with-traumatized-children-part-2-patrick-tomlinson-2014/51
van der Kolk, B. A. (2005) Developmental Trauma Disorder: Toward a Rational Diagnosis for Children with Complex Trauma Histories, in Psychiatric Annals, 35(5), 401-408
van der Kolk, B.A. and McFarlane (2007) Conclusions and Future Directions, in Traumatic Stress: The Effects of Overwhelming Experience on Mind, Body and Society New York: The Guildford Press
van der Kolk, B. (2014) The Body Keeps the Score: Brain, Mind and Body in the Healing of Trauma, Viking: New York
Wall, S., Redshaw, S. and Edwards, K. (2013) Beyond Containment: Driving Change in Residential Care: A Queensland, Australia Model of Therapeutic Residential Care, in Scottish Journal of Residential Child Care, Vol.12, No.1 https://www.celcis.org/files/7714/3565/4480/2013-vol12-no1-wall-beyondcontainment.pdf
Ward, A. (2004), Assessing and Meeting Children’s Emotional Needs, Lecture notes presented at the Therapeutic Childcare Study Day, University of Reading
Ward, A., Kasinski, K., Pooley, J., and Worthington, A. (2003) Therapeutic Communities for Children and Young People, London: Jessica Kingsley
Warner Report (1992) Choosing with Care - The Report of the Committee of Inquiry into the Selection, Development and Management of Staff in Children's Homes, HMSO
White, C. (2018) Paying Attention: The Most Exhausting Part of Parenting with ACEs! Attachment & Trauma Network, Inc, www.attachmenttraumanetwork.org/paying-attention-the-most-exhausting-part-of-parenting-with-aces/
Files
- Download a PDF of this Article
- Download a Free PDF of an Article on the International Research
- Download a free PDF of PowerPoint on International Research
- Download a Free PDF on the Co-creation of Therapeutic Models
- Download a Free PDF of Article - Therapeutic Model Development: Creativity Ownership Authority
- Download a Free PDF of Briefing Summary - Therapeutic Model Development: Creativity Ownership Author
Please leave a comment
Next Steps - If you have a question please use the button below. If you would like to find out more
or discuss a particular requirement with Patrick, please book a free exploratory meeting
Ask a question or
Book a free meeting